Definitions in the Sepsis Spectrum
- The terminology and definitions for systemic inflammation and sepsis have evolved, with current pediatric intensive care protocols defining them as follows:
| Clinical Condition | Definition & Key Features |
|---|---|
| Systemic Inflammatory Response Syndrome (SIRS) | * A hyperinflammatory state that may or may not be associated with a documented infection. * It represents a cytokine storm syndrome characterized by unregulated inflammation and potentially lethal organ system involvement. |
| Sepsis | * Defined as a life-threatening organ dysfunction caused by a dysregulated host response to an infection. |
| Severe Sepsis (Sepsis Associated Organ Dysfunction) | * Modern guidelines often refer to this state as “sepsis associated organ dysfunction”. * It is defined as a severe infection leading to cardiovascular and/or non-cardiovascular organ dysfunction. |
| Septic Shock | * Defined as a severe infection leading to cardiovascular dysfunction, which includes the presence of hypotension, the need for treatment with a vasoactive medication, or impaired perfusion. * Pathophysiologically, it manifests as a complex combination of hypovolemic, distributive, and cardiogenic shock. |
Criteria for Organ Dysfunction in Sepsis
- To identify sepsis and severe sepsis, organ dysfunction is categorized using specific clinical and laboratory parameters:
| Organ System | Dysfunction Criteria |
|---|---|
| Respiratory | * PaO2 / FiO2 < 300 (in the absence of cyanotic heart disease or preexisting lung disease). * PaCO2 > 65 mm Hg, or a 20 mm Hg increase over baseline PaCO2. * Proven need for > 50% FiO2 to maintain oxygen saturation ≥ 92%. * Need for non-elective invasive or non-invasive mechanical ventilation. |
| Neurologic | * Glasgow Coma Score ≤ 11. * Acute change in mental status with a decrease in the Glasgow Coma Score of ≥ 3 points from an abnormal baseline. |
| Hematologic | * Platelet count < 80,000/mm³ or a decline of 50% from the highest value recorded over the past 3 days. * International Normalized Ratio (INR) > 2. |
| Renal | * Serum creatinine ≥ 2 times the upper limit of normal for age, or a 2-fold increase in baseline creatinine. |
| Hepatic | * Total bilirubin ≥ 4 mg/dl (not applicable for newborns). * ALT ≥ 2 times the upper limit of normal for age. |
Pathophysiology of Septic Shock
- Septic shock in children is a complex pathophysiological state that occurs as a combination of hypovolemic, distributive, and cardiogenic shock mechanisms.
- Unlike adults, who typically present with low systemic vascular resistance (vasomotor paralysis), pediatric septic shock is most frequently associated with low cardiac output and high systemic vascular resistance.
- Almost 60% of pediatric patients present with this low cardiac output and high systemic vascular resistance phenotype, clinically referred to as “cold shock”.
- At the onset of tissue hypoperfusion, oxygen consumption and oxygen delivery are initially independent; however, as the organs fail to maintain optimal perfusion pressure due to reduced blood flow, oxygen delivery critically drops.
- When the cellular partial pressure of oxygen falls below critical levels, oxidative phosphorylation fails, triggering the anaerobic cascade.
- Sepsis-Induced Myocardial Dysfunction (SIMD) significantly contributes to the pathophysiology, affecting up to two-thirds of patients with sepsis and presenting either initially or during fluid resuscitation.
- Sepsis and septic shock can manifest broadly as either “cold shock” or “warm shock,” primarily differentiated by the patient’s compensatory mechanisms and vascular resistance.
| Clinical / Lab Parameters | Cold Shock | Warm Shock |
|---|---|---|
| Tachycardia | Present | Present |
| Pulses | Feeble | Bounding |
| Blood pressure | Normal or decreased (in late stages) | Normal or decreased (in late stages) with wide pulse pressure |
| Peripheries | Cool, mottled | Warm |
| Capillary Refill Time (CRT) | > 2 seconds | Flash, < 2 seconds |
| Urine output | Decreased | Decreased |
| Sensorium | Altered | Altered |
| ScvO2 | < 70% | Usually > 70% |
| Lactate/ Base deficit | Increased | Increased |
Note: Table adapted from clinical and laboratory features of ‘Cold shock’ and ‘Warm shock’.
Management of Septic Shock
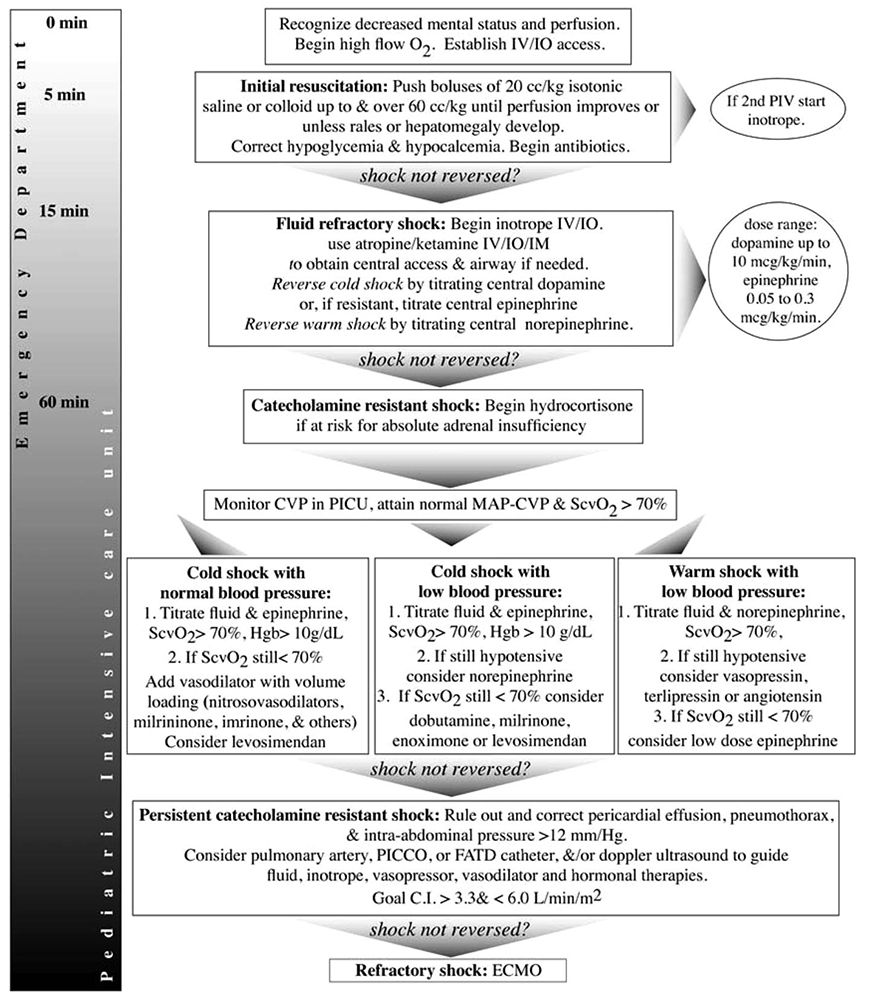 Management of Septic Shock(AHA)
Management of Septic Shock(AHA)
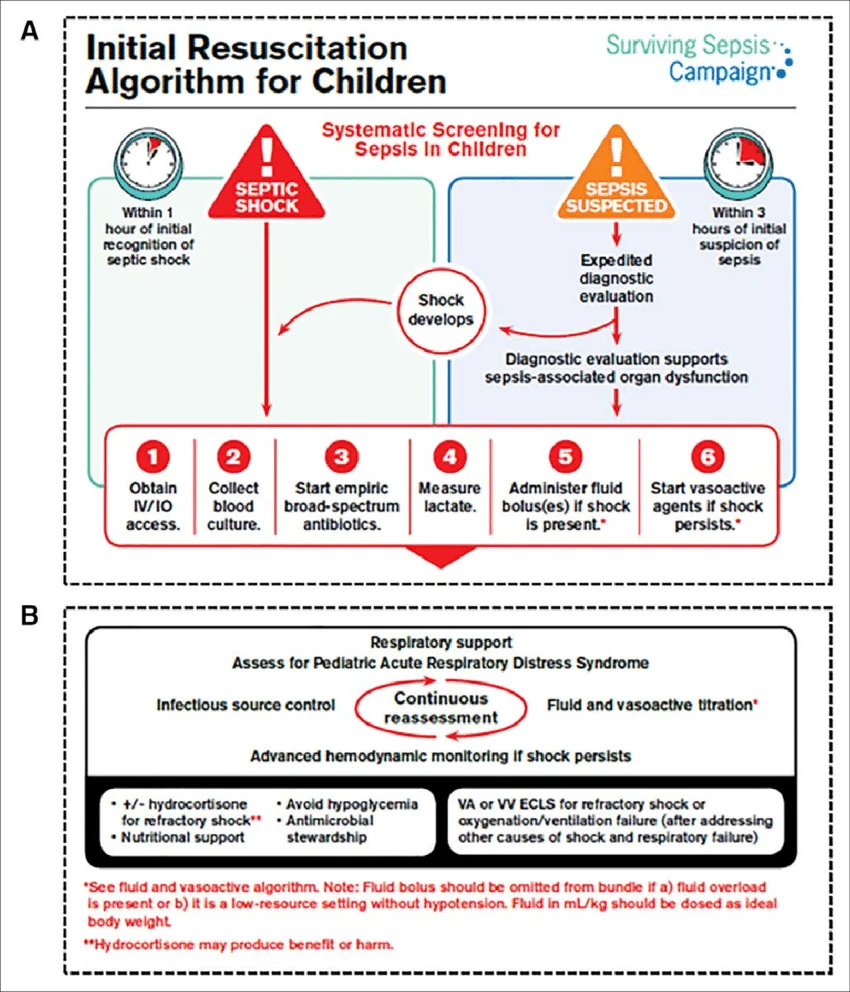 Initial Management of Septic Shock (Surving Sepsis Guidelienes)
Initial Management of Septic Shock (Surving Sepsis Guidelienes)
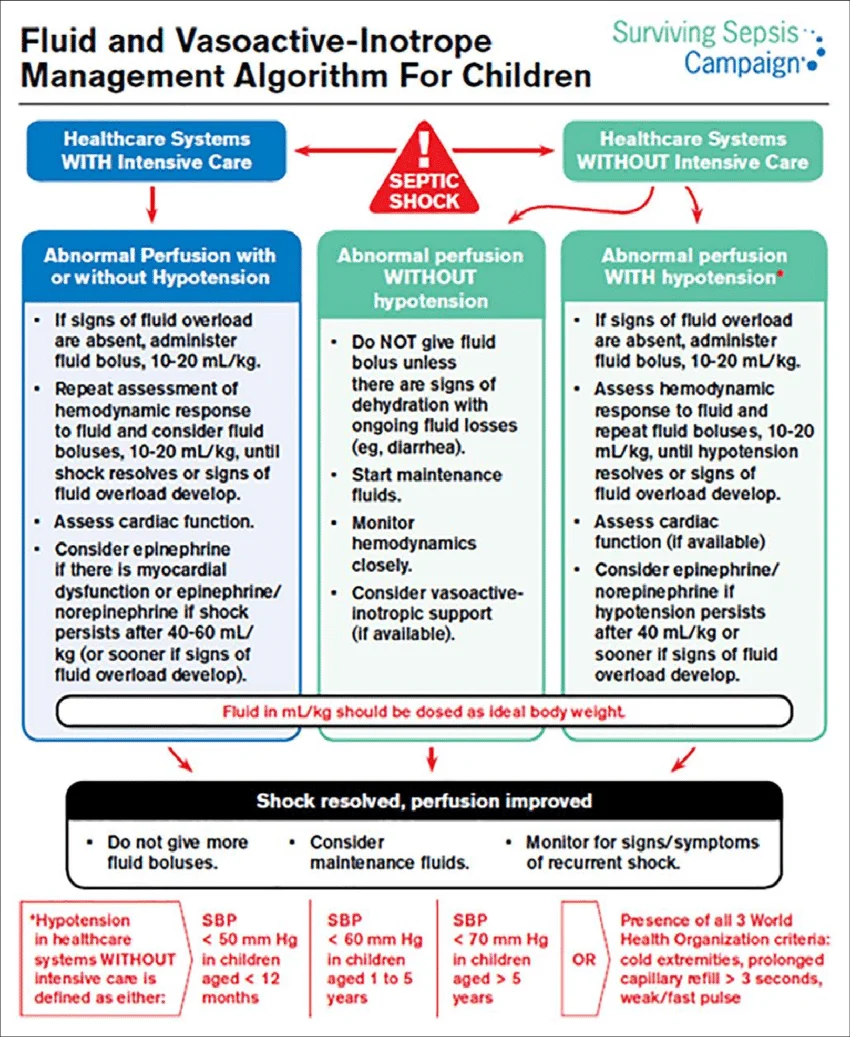 Fluid and Vasopressor in Septic Shock (Surviving Sepsis Guidelines)
Fluid and Vasopressor in Septic Shock (Surviving Sepsis Guidelines)
Early Recognition and Therapeutic Endpoints
- The initial hours following the diagnosis of sepsis and septic shock are termed the “golden hours,” and aggressive interventions during this window are heavily associated with higher survival rates and reduced multi-organ dysfunction.
- Delayed diagnosis and delays in transport or initiating treatment are major contributors to loss of the “golden hours” and poor initial management.
- Management is fundamentally based on Early Goal Directed Therapy (EGDT), which utilizes clinical and laboratory parameters to titrate therapeutic endpoints.
- The specific therapeutic endpoints targeted during the resuscitation of septic shock include:
- Normalization of the heart rate for the child’s age.
- Capillary refill time of 2 seconds.
- Well-felt dorsalis pedis pulses with no differential between peripheral and central pulses.
- Warm extremities.
- Normal range of systolic blood pressure and pulse pressure.
- Urine output > 1 ml/kg/h.
- Return to baseline mental status, tone, and posture.
- Normal range respiratory rate.
- Normal blood lactate and Superior Vena Caval oxygen saturation (ScvO2) 70%.
Stepwise Algorithmic Approach
- The First 5 minutes: Recognize decreased mental status and poor perfusion, administer high-flow oxygen, and rapidly establish intravenous (IV) or intraosseous (IO) access.
- 5 to 40 minutes (Initial Fluid Resuscitation): Infuse boluses of 20 ml/kg of isotonic saline, up to a total of 40-60 ml/kg, titrated to achieve the therapeutic goals of shock resolution.
- Throughout fluid administration, clinicians must carefully monitor the patient for signs of fluid overload, such as the development of rales or hepatomegaly.
- Correct any identified hypoglycemia and hypocalcemia immediately, and initiate broad-spectrum antibiotics (typically a third-generation cephalosporin and an aminoglycoside).
- 40 minutes (Fluid Refractory Shock): If hypotension and/or poor perfusion persist despite adequate intravascular volume repletion (40-60 ml/kg), the patient is in fluid refractory shock, warranting the initiation of vasoactive drug therapy via a central venous line.
- After 60 minutes (Catecholamine Refractory Shock): A child not responding to initial vasoactive infusions requires transfer to the Pediatric Intensive Care Unit (PICU) for invasive monitoring (CVP and arterial blood pressure) and advanced interventions, including the consideration of corticosteroids.
Fluid Resuscitation Strategies
- Isotonic crystalloids, such as Normal Saline (0.9% NaCl) or Ringer’s Lactate, are the recommended fluids for initial resuscitation due to their rapid distribution, availability, and fewer side effects.
- Current guidelines prefer balanced salt solutions (like Ringer’s Lactate) over Normal Saline to prevent hyperchloremic acidosis and acute kidney injury, except in specific conditions like raised intracranial tension or hyponatremia.
- The use of synthetic colloids (e.g., hydroxyethyl starch solutions) is strictly not recommended, as they increase the risk of acute kidney injury, coagulopathy, and mortality.
- Fluids should be administered as rapid boluses of 10-20 ml/kg over 15-20 minutes or 5-10 minutes, but they must be immediately discontinued if clinical signs of fluid overload develop (e.g., increasing liver span, jugular venous distension, pulmonary edema).
Vasoactive Medications
- Vasoactive medications are initiated for fluid refractory shock; the choice of agent is determined by the clinical phenotype (cold vs. warm shock).
- Epinephrine or norepinephrine can both be utilized as first-line agents; dopamine is an acceptable alternative if the primary agents are unavailable.
- For Cold Shock (low cardiac output, high systemic vascular resistance), reversal is attempted by titrating an epinephrine infusion.
- For Warm Shock (diffuse vasodilation, wide pulse pressure, low blood pressure), a norepinephrine infusion (0.1-1 g/kg/min) is the treatment of choice to restore vascular tone.
- Inodilators, such as milrinone, are highly indicated in children who exhibit persistent hypoperfusion, high systemic vascular resistance, and documented cardiac dysfunction despite the use of epinephrine.
- Vasopressin may be considered as a rescue therapy for patients presenting with warm shock and low blood pressure that remains entirely unresponsive to high-dose norepinephrine.
Antimicrobial Therapy and Source Control
- Timely administration of appropriate antimicrobials is a critical pillar of management; delayed administration directly correlates with increased morbidity and mortality.
- Intravenous antimicrobials must be administered within 1 hour of presentation for a child in septic shock.
- Blood cultures (at least two sets) should be obtained before initiating antibiotics, provided this does not significantly delay the antimicrobial administration.
- Source control—such as the drainage of an abscess, debridement of infected necrotic tissue, or removal of a potentially infected intravascular access device—must be evaluated and executed within 6 hours of presentation.
Corticosteroids and Host Response Interventions
- Corticosteroids are not recommended for routine use in pediatric septic shock.
- They are specifically indicated for children with catecholamine-resistant (refractory) shock who have proven or suspected adrenal insufficiency.
- The recommended regimen in fluid and catecholamine-refractory shock is intravenous Hydrocortisone (50 to 100 mg/m/dose or 1 to 2 mg/kg/dose), which should be discontinued once the patient achieves hemodynamic stability and no longer requires vasoactive support.
- Intravenous immunoglobulin (IVIG) is not recommended for routine management in pediatric sepsis or septic shock due to inadequate supporting data.
Supportive Care and Organ System Management
- Mechanical Ventilation: Early intubation and mechanical ventilation reduce the work of breathing (which can account for 15% to 30% of oxygen consumption in septic shock) and allow for the redistribution of limited cardiac output to vital organs.
- Etomidate and propofol should be avoided during intubation to prevent adrenal suppression and metabolic acidosis; Ketamine is the preferred induction agent if not contraindicated.
- Blood Products: The optimal hemoglobin threshold for transfusion in severe sepsis remains unclear, but guidelines suggest withholding RBC transfusions if the hemoglobin is 7 g/dL in hemodynamically stable children.
- Prophylactic platelet transfusions are generally indicated if counts are < 5,000/mm, or between 5,000-30,000/mm with a significant risk of bleeding; fresh frozen plasma (FFP) is reserved exclusively for patients with active bleeding or prior to invasive procedures, rather than for correcting isolated laboratory coagulopathies.
- Glycemic Control: Blood glucose should be meticulously monitored to avoid both hypoglycemia and hyperglycemia. Levels exceeding 180 mg/dl should be managed with low-dose insulin infusions, while targeting a strict normoglycemic range (e.g., <140 mg/dL) is not recommended due to the high risk of fatal hypoglycemia.
- Nutrition: Early initiation of enteral feeding (gastric over post-pyloric) is highly recommended, whereas Total Parenteral Nutrition (TPN) should be avoided during the first week of illness.