The evaluation of a child presenting with a rhythm disturbance hinges on two primary considerations: the child’s typical heart rate/rhythm for their age and the patient’s hemodynamic status (clinical condition).
Tachycardia is defined as a heart rate that is abnormally fast compared to the normal physiological heart rate for the patient’s age.
The rhythm is clinically categorized as “unstable” if the tachycardia produces signs of poor tissue perfusion, such as weak pulses, hypotensive shock, respiratory distress, or altered consciousness.
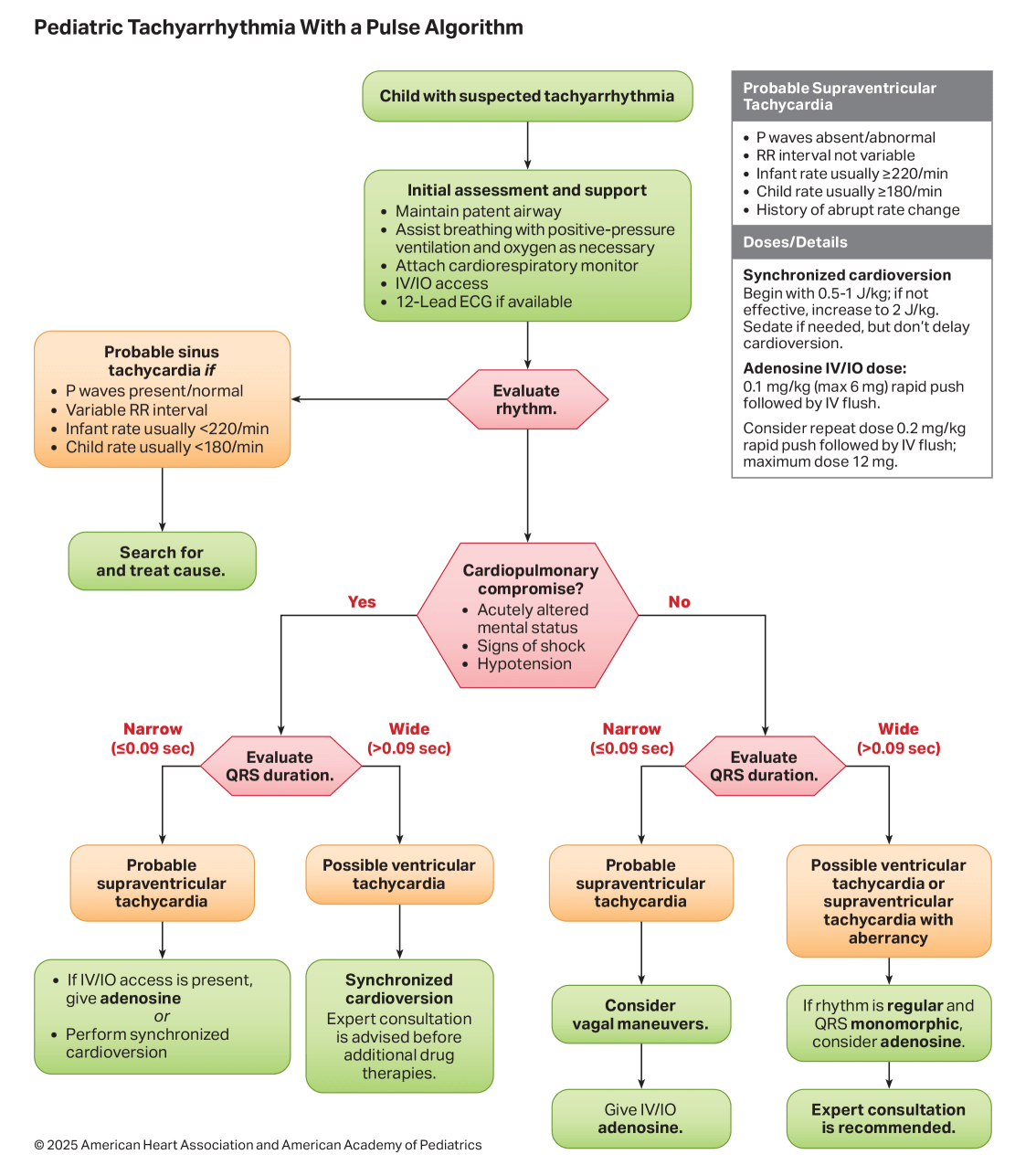
Once a pulse is confirmed to be present, tachyarrhythmias are classified based on the width of the QRS complex on the electrocardiogram (ECG).
Narrow Complex Tachycardia (QRS ≤ 0.09 seconds): Includes Sinus Tachycardia (ST), Supraventricular Tachycardia (SVT), and Atrial Flutter.
Wide Complex Tachycardia (QRS > 0.09 seconds): Includes Ventricular Tachycardia (VT) and SVT with aberrant intraventricular conduction.
Differentiating Narrow Complex Tachycardias (ST vs. SVT)
Distinguishing between Sinus Tachycardia (ST) and Supraventricular Tachycardia (SVT) is a critical step in the narrow-complex algorithm, guided by clinical history and ECG characteristics.
Parameter
Sinus Tachycardia (ST)
Supraventricular Tachycardia (SVT)
Heart Rate (Infants)
Usually < 220 beats/min
Usually ≥ 220 beats/min
Heart Rate (Children)
Usually < 180 beats/min
Usually ≥ 180 beats/min
History
Gradual onset; compatible with a known cause (e.g., fever, pain, volume loss)
Abrupt onset; vague, non-specific history or symptoms of congestive heart failure
P-wave
Present and normal (upright in leads I/aVF)
Absent or abnormal (negative in leads II/III/aVF)
R-R Interval
Variable with level of activity
Constant (Not variable)
P-R Interval
Constant
Variable
Management of Hemodynamically Unstable Tachycardia (Poor Perfusion)
Immediate intervention is mandated for any tachyarrhythmia presenting with signs of hemodynamic instability and compromised perfusion.
Narrow Complex (Unstable SVT): Synchronized cardioversion is the definitive therapy of choice and must be administered as soon as possible.
The initial dose for synchronized cardioversion is 0.5 to 1 J/kg.
If the first shock is unsuccessful, the subsequent dose is escalated to 2 J/kg.
A rapid dose of Adenosine may be attempted first to determine if the rhythm is SVT, provided that its administration does not delay the electrical cardioversion.
Wide Complex (Unstable VT with Pulse): Unstable wide-complex tachycardia is treated identically with synchronized cardioversion (0.5 to 1 J/kg, escalating to 2 J/kg).
If the wide-complex tachycardia is refractory to synchronized shocks, or if it recurs quickly, pharmacological therapy with intravenous Amiodarone or Lidocaine should be administered.
If at any point the patient loses their pulse, the provider must immediately commence cardiopulmonary resuscitation (CPR) and shift to the pulseless arrest (defibrillation) algorithm.
Management of Hemodynamically Stable Tachycardia (Adequate Perfusion)
For patients maintaining adequate perfusion and blood pressure, the approach is stepwise and pharmacological, guided by the QRS width.
Stable Narrow Complex (Probable ST): Identify and aggressively treat the underlying reversible causes, such as hypovolemia, fever, or pain (the “Hs and Ts”).
Stable Narrow Complex (Probable SVT):
Vagal maneuvers should be attempted first, provided they do not unduly delay chemical cardioversion.
For infants and young children, ice applied to the face (without occluding the airway) is utilized.
For older children, Valsalva maneuvers (e.g., blowing through an obstructed straw) or carotid sinus massage are safe and effective.
If vagal maneuvers fail, Adenosine is the pharmacological drug of choice.
Stable Wide Complex (Probable VT):
An expert cardiology consultation is highly recommended.
Pharmacological cardioversion is achieved using an infusion of Amiodarone.
Alternative agents include Procainamide or a Lidocaine bolus followed by an infusion.
Pharmacological Agents and Dosages
Adenosine: Administered via rapid intravenous push using a ‘two-syringe’ technique (drug followed immediately by a rapid ≥ 5 ml normal saline flush). The initial dose is 0.1 mg/kg (maximum first dose 6 mg). If there is no response, the dose is doubled to 0.2 mg/kg (maximum second dose 12 mg).
Amiodarone: Administered as an intravenous infusion of 5 mg/kg given slowly over 20 to 60 minutes (maximum 300 mg per dose). It can be repeated up to a total daily dose of 15 mg/kg (maximum 2.2 g in 24 hours).
Procainamide: Administered as an intravenous infusion of 15 mg/kg slowly over 30 to 60 minutes. Note: Extreme caution must be exercised if administering both Amiodarone and Procainamide due to the compounded risk of severe QTc prolongation.
Lidocaine: Administered as a 1 mg/kg intravenous bolus, which can be followed by a continuous infusion of 20 to 50 μg/kg/min.