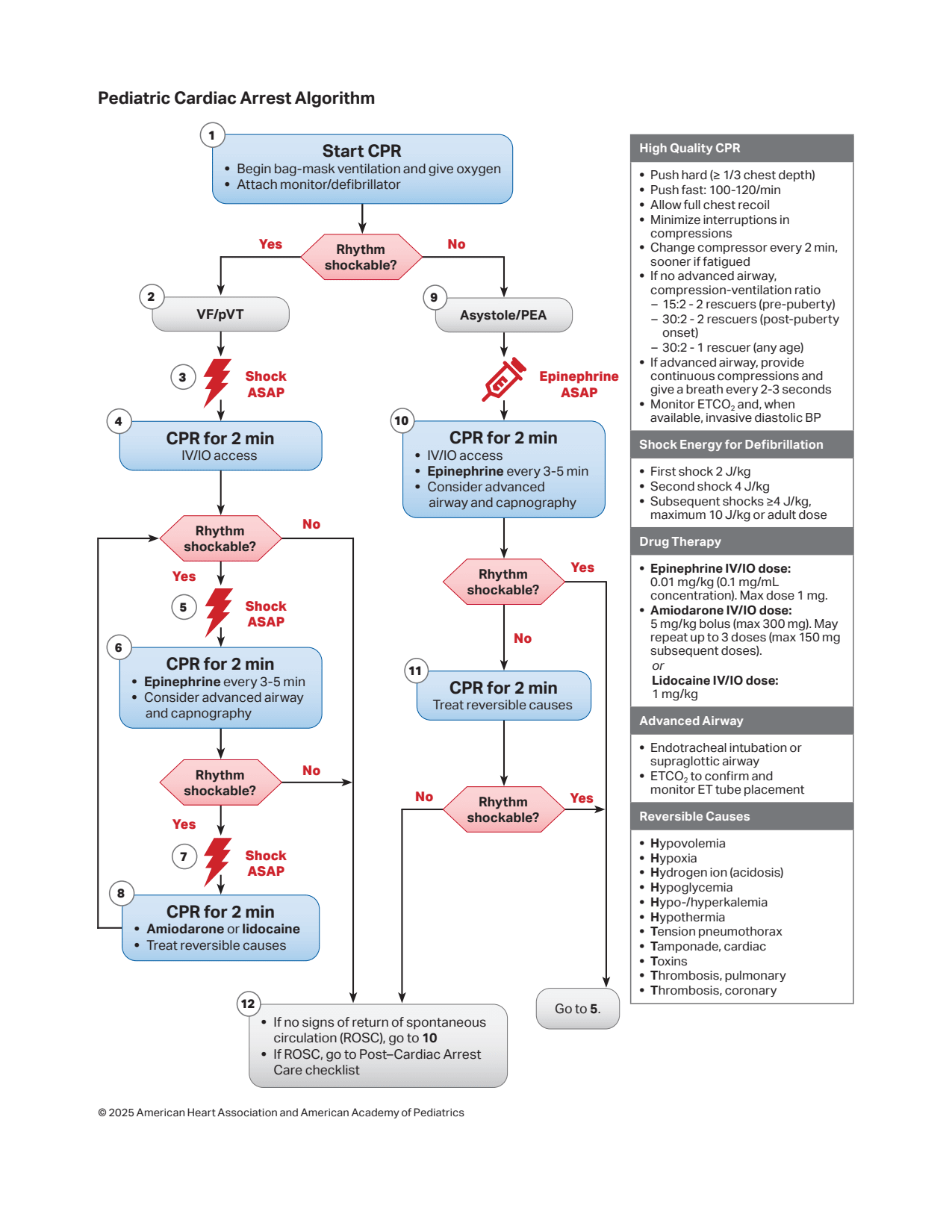
The pediatric cardiac arrest algorithm is a structured, stepwise approach utilized for the immediate management of a child presenting with absent or ineffective cardiac mechanical activity.
Upon detecting a pulseless arrest, the initial intervention is the prompt initiation of high-quality cardiopulmonary resuscitation (CPR) following the C-A-B (Compressions-Airway-Breathing) sequence.
Simultaneously, supplemental oxygen must be started, and a cardiac monitor or defibrillator must be attached to identify the underlying arrest rhythm.
The management pathway subsequently diverges based on whether the cardiac rhythm is defined as “shockable” or “non-shockable”.
Management of Shockable Rhythms (VF / Pulseless VT)
Ventricular fibrillation (VF) and pulseless ventricular tachycardia (VT) are categorized as shockable rhythms.
Immediately deliver the first defibrillation shock at a dose of 2 J/kg.
Resume CPR immediately after the shock and continue for 2 minutes (or 5 cycles) without pausing for a pulse check.
After 2 minutes, perform a rhythm and pulse check; if the rhythm remains shockable, deliver a second shock at 4 J/kg.
Resume CPR immediately for another 2 minutes and administer the first dose of Adrenaline (0.01 mg/kg IV/IO).
Adrenaline administration should be repeated every 3 to 5 minutes throughout the duration of the cardiac arrest.
If the rhythm continues to be shockable at the next check, deliver a third shock at 4 J/kg (or escalate up to a maximum of 10 J/kg).
Resume CPR immediately and administer an antiarrhythmic drug, preferring either Amiodarone (5 mg/kg bolus) or Lidocaine (1 mg/kg).
Continuously look for and treat reversible underlying causes (the Hs and Ts) during the resuscitation cycles.
Management of Non-Shockable Rhythms (Asystole / PEA)
Asystole and Pulseless Electrical Activity (PEA) are the most common arrest rhythms in children and are managed without defibrillation.
Immediately resume and continue high-quality CPR with minimal interruptions.
Administer Adrenaline at a standard dose of 0.01 mg/kg IV/IO (0.1 ml/kg of 1:10,000 solution) as soon as vascular access is established.
Repeat the Adrenaline dose every 3 to 5 minutes.
Perform a rhythm and pulse check every 2 minutes.
If the rhythm becomes organized and a pulse is present, proceed to post-resuscitation or Return of Spontaneous Circulation (ROSC) care.
If the rhythm changes to a shockable rhythm at any point, switch to the shockable algorithm and deliver a defibrillation shock.
Concurrently search for and aggressively manage any reversible causes.
High-Quality CPR Parameters
The efficacy of the arrest algorithm relies heavily on maintaining high-quality CPR metrics throughout the resuscitation effort.
Parameter
Recommendation for Infants and Children
Compression Rate
100 to 120 compressions per minute.
Compression Depth
Compress at least one-third of the anterior-posterior diameter of the chest (approximately 4 cm in infants 5 cm in children).
Chest Recoil
Allow full chest recoil between compressions to optimize cardiac filling and venous return.
Minimizing Interruptions
Limit interruptions in chest compressions to less than 10 seconds for rhythm checks or shock delivery.
Compression-to-Ventilation Ratio
30:2 for a single rescuer; 15:2 when two rescuers are present.
Ventilation with Advanced Airway
Provide continuous compressions without pausing for breaths; deliver 1 breath every 6 seconds (10 breaths/min).
Reversible Causes of Cardiac Arrest (Hs and Ts)
Identifying and treating the precipitating cause is critical for successful resuscitation and must be integrated continuously into the algorithm.