The initial evaluation of a pediatric patient with a rhythm disturbance must focus on the child’s heart rate, rhythm, and clinical hemodynamic status.
Bradycardia is defined as a heart rate slower than normal for the patient’s age.
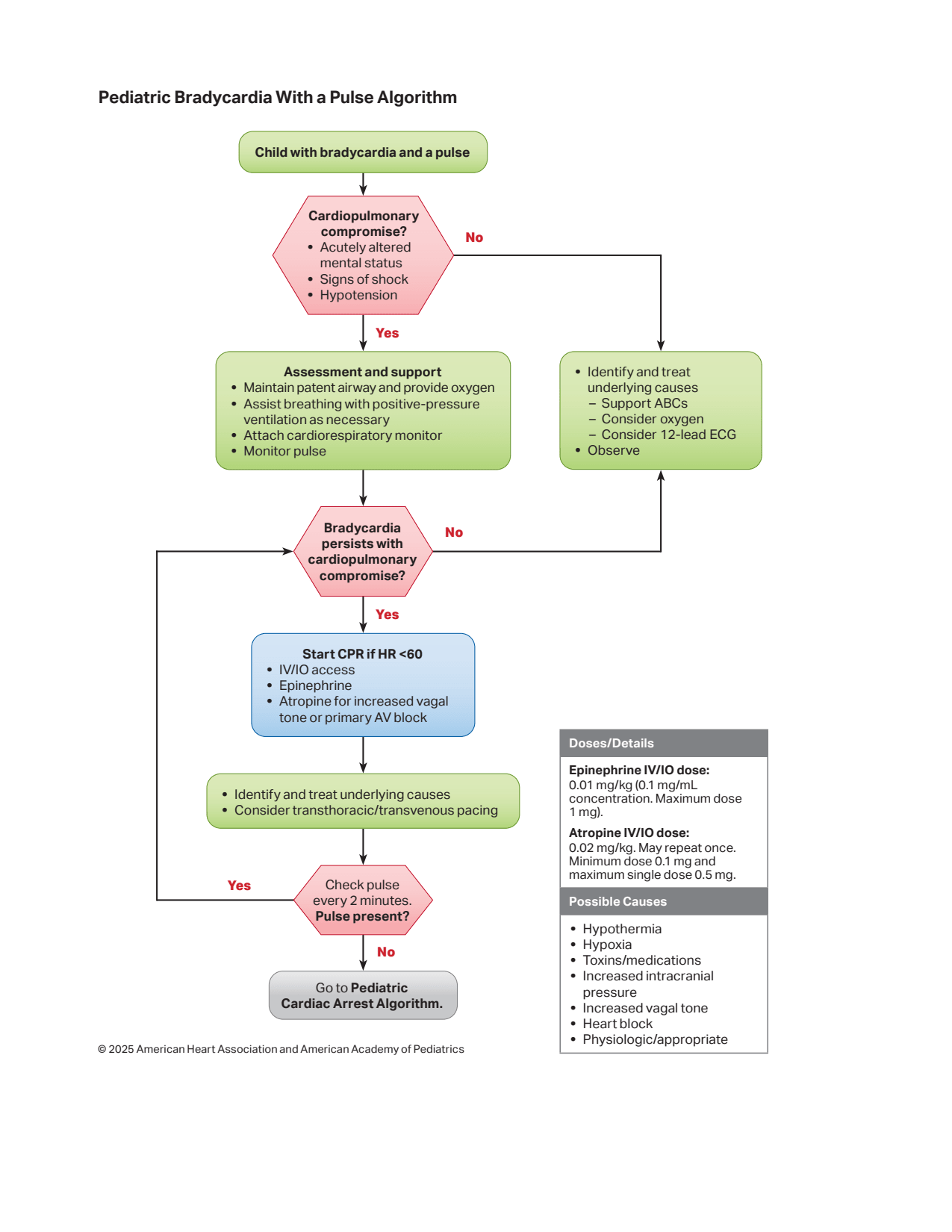
The emergency management of bradycardia is dictated by its hemodynamic consequences.
If bradycardia causes cardiorespiratory compromise, the initial step is to support the airway, breathing, and circulation (ABC) as required, administer supplemental oxygen, and attach a cardiac monitor or defibrillator.
After securing the ABCs, the clinician must reassess the patient; if pulses, perfusion, and respirations normalize, no immediate emergency treatment is required, and the child should be continuously monitored while proceeding with further evaluation.
If at any point the patient loses their pulse and develops pulseless arrest, the provider must immediately initiate cardiopulmonary resuscitation (CPR).
Management of Bradycardia with Poor Perfusion
If the heart rate remains <60 beats per minute and is associated with poor systemic perfusion despite effective ventilation and oxygen administration, the provider must immediately start chest compressions.
During this phase, it is critical to continue supporting the airway, maintaining ventilation, and providing oxygenation alongside chest compressions.
Pharmacological Interventions
Epinephrine is the primary drug of choice for pediatric bradycardia associated with poor perfusion that does not respond to oxygenation and ventilation.
Atropine is specifically indicated when bradycardia is caused by increased vagal tone (e.g., vagal stimulation) or a primary atrioventricular (A-V) block.
If the bradycardia persists or responds only transiently to bolus medications, a continuous infusion of Epinephrine (0.1−0.3μg/kg/min) or Isoproterenol should be considered.
Medication
Route
Recommended Dose
Frequency & Remarks
Epinephrine
IV / IO
0.01 mg/kg (0.1 ml/kg of 1:10,000 solution)
Repeat every 3 to 5 minutes.
Epinephrine
Endotracheal (ET)
0.1 mg/kg (0.1 ml/kg of 1:1,000 solution)
Repeat every 3 to 5 minutes.
Atropine
IV / IO
0.02 mg/kg (No minimum dose)
Maximum single dose is 0.5 mg for a child and 1 mg for an adolescent; repeat once in 5 minutes if no response (Maximum total dose: 1 mg for child, 2 mg for adolescent).
Atropine
Endotracheal (ET)
0.04 to 0.06 mg/kg
Repeat once in 5 minutes if there is no response.
Advanced Interventions (Pacing)
Emergency transcutaneous cardiac pacing can be a life-saving measure if the bradycardia is caused by complete heart block or sinus node dysfunction that remains unresponsive to ventilation, oxygenation, chest compressions, and medications.
Pacing is particularly useful when the condition is associated with congenital or acquired heart disease.
Cardiac pacing is not effective and is not indicated for asystole or for bradycardia that is secondary to a post-arrest hypoxic/ischemic myocardial insult or respiratory failure.
Identification and Treatment of Reversible Causes
While actively managing the bradyarrhythmia, the clinician must continuously look for and treat any underlying contributing factors, which are easily remembered by the “Hs” and “Ts” mnemonic.