Paracetamol (acetaminophen) is a widely used analgesic and antipyretic agent, and its toxicity is the most common cause of acute liver failure in the Western world.
In therapeutic use, paracetamol is primarily detoxified in the liver via glucuronidation and sulfation into nontoxic products.
A small percentage (approximately 5%) is metabolized by the hepatic cytochrome P450 enzyme (CYP2E1) into a highly reactive intermediate metabolite, N-acetyl-p-benzoquinoneimine (NAPQI).
Normally, NAPQI is immediately conjugated with glutathione to form a nontoxic mercapturic acid conjugate and excreted harmlessly.
In an overdose scenario, glutathione stores become rapidly depleted, leaving free NAPQI to covalently bind with hepatic macromolecules, ultimately producing severe hepatocellular necrosis.
The acute toxic dose of paracetamol in children is generally >200 mg/kg.
Repeated administration of supratherapeutic doses (>90 mg/kg/day for consecutive days) can also lead to significant hepatic injury, particularly in the setting of fever, dehydration, poor nutrition, or other conditions that reduce baseline glutathione stores.
Clinical Stages of Toxicity
The clinical manifestations of paracetamol intoxication follow a classic four-stage progression.
Patients will either recover completely or progress to fulminant hepatic failure depending on the ingested dose and the timing of antidotal therapy.
Stage
Time After Ingestion
Clinical Characteristics
Laboratory Findings
Stage 1
0−24 hours
Asymptomatic, or nonspecific symptoms such as anorexia, nausea, vomiting, and malaise
Laboratory tests are typically normal except for the elevated paracetamol level
Stage 2
24−48 hours
Resolution of earlier gastrointestinal symptoms; onset of right upper quadrant abdominal pain and tenderness
Evidence of elevated liver transaminases (AST > ALT) and elevated INR
Stage 3
3−5 days
Anorexia, nausea, vomiting; development of liver failure and multiorgan system dysfunction; potential for death or start of recovery
Peak transaminase elevation
Stage 4
4 days to 2 weeks
Recovery phase with resolution of clinical symptoms
Improvement and eventual resolution of hepatic functions; clinical recovery precedes histologic recovery
Diagnostic Evaluation
The diagnosis of paracetamol toxicity cannot rely on clinical symptoms alone, as patients in the early stages are often entirely asymptomatic.
A serum paracetamol level must be checked in all patients presenting with an intentional exposure or suspected overdose, optimally obtained 4 hours after the reported time of ingestion.
Levels obtained <4 hours post-ingestion are difficult to interpret and cannot reliably estimate the potential for hepatotoxicity.
The normal therapeutic level of paracetamol is 10−20μg/mL.
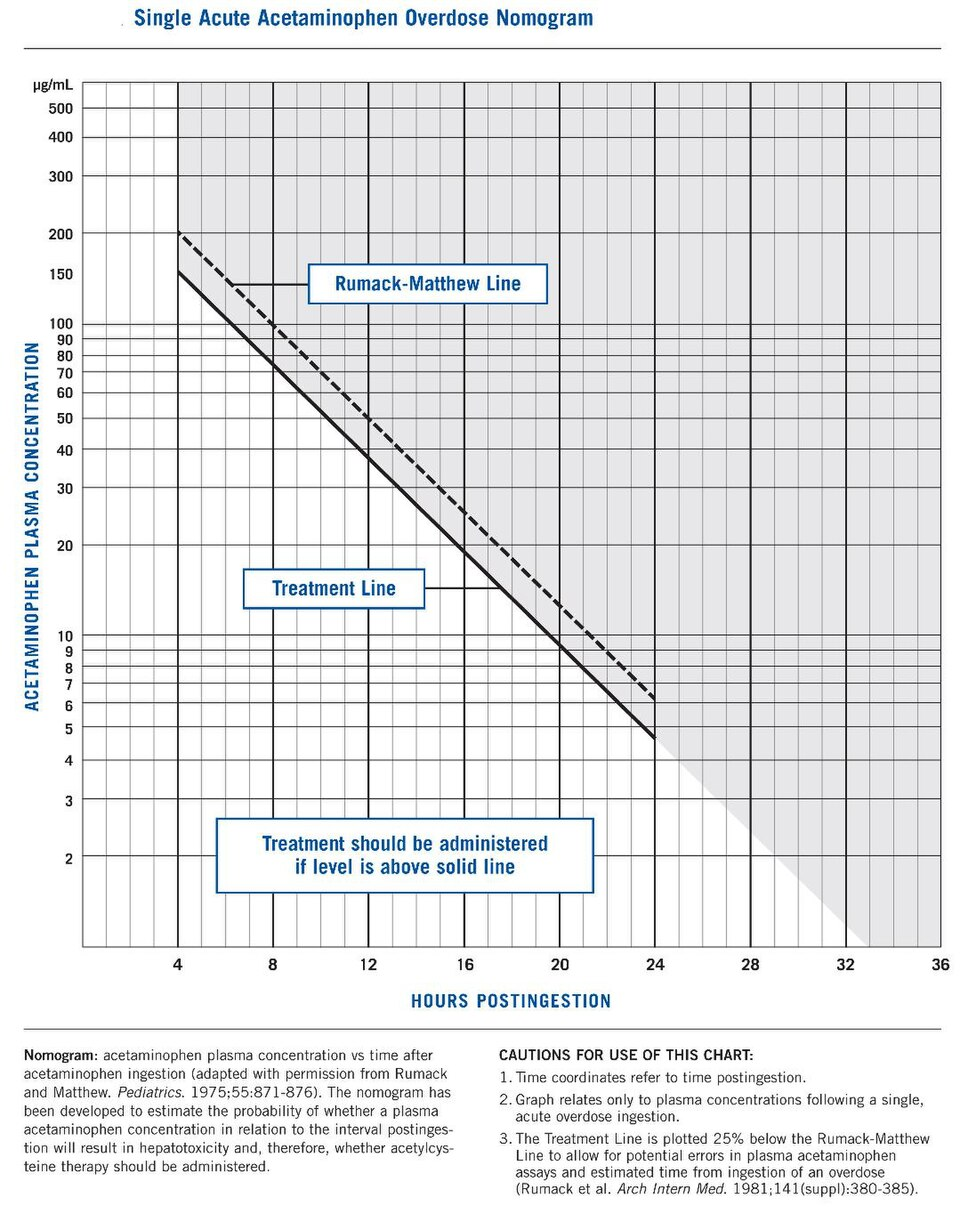
The 4-hour or subsequent levels are plotted on the Rumack-Matthew nomogram to guide treatment decisions.
The treatment line on the Rumack-Matthew nomogram is typically plotted 25% below the standard line to allow for estimated errors in blood assays and timing of the overdose.
The nomogram is strictly intended for single acute ingestions with a known time of ingestion and cannot be utilized for chronic exposures, repeated doses, ingestions >24 hours old, or when co-ingestants slow gastrointestinal motility.
Baseline laboratory evaluations should always include hepatic transaminases (AST and ALT), total bilirubin, renal function tests (creatinine, blood urea nitrogen), and coagulation parameters (INR).
Emergency Management and Decontamination
Initial management involves stabilization of airway, breathing, and circulation, along with rapid assessment of mental status.
Gastric lavage may be considered if the patient presents within 4 hours of a massive ingestion.
Administration of single-dose activated charcoal is recommended if the patient presents within 1−2 hours of ingestion, provided the patient is alert and has an intact, protected airway.
While activated charcoal binds to paracetamol, its use should not delay the administration of the specific antidote, and it carries the risk of inducing vomiting.
Specific Antidote Therapy (N-Acetylcysteine)
N-acetylcysteine (NAC) acts as a precursor for glutathione synthesis, directly reducing the incidence of hepatotoxicity if administered promptly.
If administered within 8 hours of the overdose, NAC is highly effective, and mortality from liver failure is virtually eliminated.
Delays in NAC administration beyond the 8-hour window increase the risk of acute liver failure, requiring empirical NAC therapy to be started pending laboratory results for late presentations.
NAC can be administered via oral or intravenous routes, both of which are considered equally efficacious for systemic detoxification.
Intravenous NAC is specifically indicated in cases of intractable vomiting, established hepatic failure, and pregnancy.
Administration of intravenous NAC (especially during the loading dose) may cause non-IgE-mediated anaphylactoid reactions, which are managed by temporarily stopping the infusion, administering diphenhydramine or epinephrine, and restarting at a slower rate.
Intravenous NAC may cause mild, transient laboratory elevations in the INR (range 1.2−1.5) due to assay interference.
Route
Regimen
Dosage and Administration
Oral
72-hour protocol
140 mg/kg loading dose, followed by 70 mg/kg every 4 hours for 17 additional doses
Intravenous
21-hour protocol
150 mg/kg over 1 hour (loading), followed by 50 mg/kg over 4 hours, then 100 mg/kg over 16 hours
Categorized Management Approach
Treatment pathways are categorized based on the presentation type, transaminase levels, and liver function.
Category
Clinical / Lab Status
Management Strategy
Category 1: Prophylactic
Normal transaminases
If levels fall in the “possible/probable toxicity” range on the Rumack-Matthew nomogram, start NAC. If time of ingestion is unknown, treat until paracetamol is undetectable.
Category 2: Hepatic Injury
Elevated transaminases (AST > ALT) and rising INR
Indicates hepatocellular necrosis. NAC is mandatory. Discontinue NAC only when transaminases and INR have peaked and are actively declining.
Category 3: Acute Liver Failure
Fulfills King’s College Criteria for transplant referral
Requires intensive care and urgent evaluation for liver transplantation.
Category 4: Repeated Supratherapeutic
Multiple doses >90 mg/kg/day; Nomogram not applicable
If asymptomatic with normal AST and APAP <10μg/mL, no therapy is needed. If APAP is elevated but AST is normal, give NAC until APAP is undetectable. If AST is elevated or patient is symptomatic (jaundice, vomiting), empirically start NAC.
Indications for Liver Transplantation
The King’s College criteria are the standard prognostic tool used for deciding referral for liver transplantation in paracetamol-induced acute liver failure.
Transplantation referral is indicated if there is severe acidemia with a serum pH <7.3following adequate fluid resuscitation.
Alternatively, referral is strictly indicated if all three of the following criteria are met:
severe coagulopathy with an INR > 6.0 (or >6.5),
severe renal dysfunction with serum creatinine > 3.3 mg/dL (or >3.4 mg/dL), and
grade III or IV hepatic encephalopathy.
A serum lactic acid level >3 mmol/L after intravenous fluid resuscitation adds significant sensitivity and specificity for predicting mortality and the need for a transplant.
The absolute peak value of transaminase elevation does not determine the need for liver transplantation.
Differential Diagnosis of Acute Liver Failure in Children
In children presenting with features of hepatotoxicity and encephalopathy, other conditions should be rapidly considered, especially if the paracetamol level is non-toxic.
Acute infectious hepatitis (Hepatitis A, B, E) remains the most common cause of acute liver failure in Indian children.
Metabolic liver diseases, such as Wilson disease (indicated by Kayser-Fleischer rings, low ceruloplasmin, Coombs-negative hemolytic anemia) and Galactosemia, should be considered.
Autoimmune hepatitis, characterized by positive ANA, SMA, or LKM antibodies, may present acutely with a hepatitis-like picture.
Other drug-induced hepatotoxicities, such as valproate toxicity or idiosyncratic reactions to anti-tuberculosis drugs (isoniazid, rifampicin), must be systematically ruled out.