Organophosphates are commonly used pesticide agents and represent a frequent cause of severe accidental and intentional poisoning in children and adolescents, particularly in developing nations.
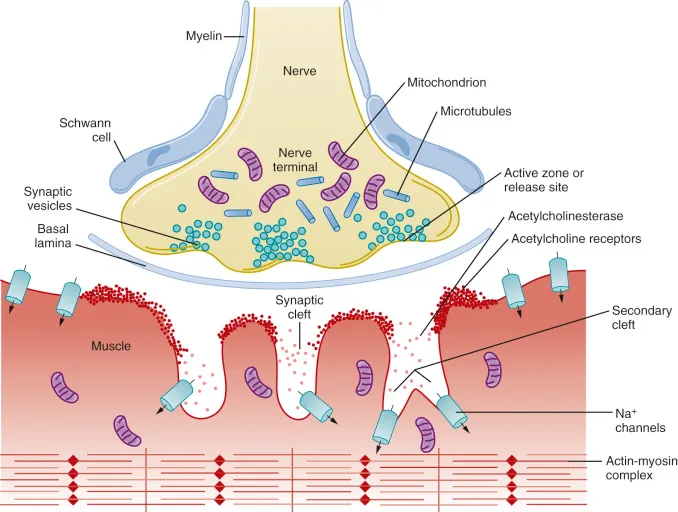
Organophosphate compounds (OPCs) cause toxicity by inhibiting the enzyme acetylcholinesterase (AChE), which is responsible for the normal degradation of acetylcholine (ACh).
The inhibition occurs when the OPC phosphorylates the serine hydroxyl residue on the AChE enzyme.
This creates an irreversible covalent bond that permanently inactivates the enzyme, a time-dependent process known clinically as “aging”.
In contrast, related carbamate pesticides reversibly bind to AChE.
The inactivation of AChE leads to a massive accumulation of ACh at nerve synapses and neuromuscular junctions throughout the body.
The excess ACh results in the severe overstimulation of both nicotinic and muscarinic receptors in the central and peripheral nervous systems, producing a cholinergic crisis
Clinical Manifestations
The severity and onset of symptoms depend upon the route of exposure, the duration of exposure, and the absorbed dose.
Acute organophosphate poisoning is classically characterized by three distinct clinical phases: acute cholinergic crisis, intermediate syndrome, and delayed neuropathy.
1. Acute Cholinergic Crisis
This is the initial phase characterized by an overwhelming autonomic storm due to muscarinic and nicotinic receptor overstimulation.
Severe poisoning can rapidly progress to coma and respiratory failure.
The clinical features are broadly divided into muscarinic, nicotinic, and central nervous system effects:
This phase develops in some patients while they are recovering from the initial acute cholinergic crisis.
It is primarily characterized by the development of respiratory failure due to diaphragmatic and respiratory muscle weakness.
3. Delayed Neuropathy
This is a late-onset phase that occurs weeks after the initial exposure.
It manifests as delayed polyneuropathy and a range of chronic neuropsychiatric symptoms
Diagnosis
The diagnosis of organophosphate poisoning is primarily clinical, based on the characteristic cholinergic signs and the presence of a garlic-like odor from the patient or their bodily fluids.
Laboratory confirmation is achieved by demonstrating reduced butyrylcholinesterase activity in plasma or reduced acetylcholinesterase activity in the blood.
Enzyme activity levels measuring <10% of normal values indicate severe poisoning.
Emergency treatment must be initiated immediately based on clinical suspicion and should never be delayed while awaiting the results of cholinesterase assays.
Management
The management of organophosphate toxicity is a medical emergency that involves immediate resuscitation, thorough decontamination, and the expeditious administration of specific antidotes.
Management Step
Specific Interventions
Initial Stabilization (ABCs)
Check airway, breathing, and circulation. Provide 100% oxygen and mechanical ventilation as indicated for respiratory failure or excessive secretions. Avoid using succinylcholine for rapid sequence intubation, as it is metabolized by the same inhibited cholinesterase enzymes and will cause prolonged paralysis.
Decontamination
Immediate dermal and ocular decontamination is critical. Remove all clothing and thoroughly wash the exposed skin with soap and water. Activated charcoal or gastric lavage is generally not beneficial as these liquid agents are absorbed very rapidly.
Atropine Therapy
Atropine acts as an antidote by competitively antagonizing muscarinic acetylcholine receptors. Administer an initial intravenous (IV) or intraosseous (IO) bolus of 0.02−0.1 mg/kg. Assess pupil size, sweating, heart rate, and blood pressure. If there is no improvement, repeat boluses of 0.05 mg/kg every 5 to 10 minutes. The therapeutic endpoint (atropinization) is reached when the heart rate is appropriate for age, systolic blood pressure is >5th centile, and chest auscultation is clear of bronchorrhea. Once stable, initiate a continuous IV infusion of atropine at 10−20% of the cumulative bolus dose per hour.
Pralidoxime (PAM) Therapy
Pralidoxime facilitates the reactivation of acetylcholinesterase by breaking the bond between the enzyme and the toxin before “aging” occurs. Administer a loading dose of 25−50 mg/kg IV over 20-30 minutes. Follow with a continuous infusion of 10−20 mg/kg/hr in saline. PAM infusion should continue until atropine is no longer required for 12-24 hours and the patient is successfully extubated.
Supportive Care
Provide sedation with benzodiazepines to manage atropine-induced agitation or organophosphate-induced seizures. Continuously monitor fluid balance, electrolytes, and cardiovascular status.